Tailored by the Trace: How Measurable Residual Disease is Helping Guide Hematology Treatment



by Marc Astick, Associate Scientific Director and Rebecca Lamb, Senior Group Director
Ask experts in hematology what they’re working towards and you’re likely to hear one common theme: adaptive care. To be able to read disease more precisely and shape treatment around the patient to achieve the best possible outcomes.1 This is an aim across this fast-moving field that will run through EHA this June.2 For us, one topic that really captures that ambition is measurable (or minimal) residual disease, or MRD. Simply put, MRD is the trace of cancer that lingers after treatment.1
But how do we find this trace, and why is it important?
MRD is assessed by reading the proteins on a cell’s surface (using flow cytometry), tracing its genetic fingerprint or catching tumor DNA shed into the blood (using next-generation sequencing or polymerase chain reaction1). With these techniques it is possible to spot a single cancer cell in anywhere from 100,000 to 1 million other cells, providing a fine lens, that moves beyond the limit of traditional response assessment on how deep a response to treatment is. 3,4 This depth matters: across hematological malignancies, MRD has emerged as a strong prognostic indicator. MRD-negative patients may have better survival rates and a lower risk of relapse compared with those with detectable disease.5–7
What’s changed is how precisely we can read it, and the challenge now facing the field is how this impacts clinical decision making.4
How does MRD impact patient care?
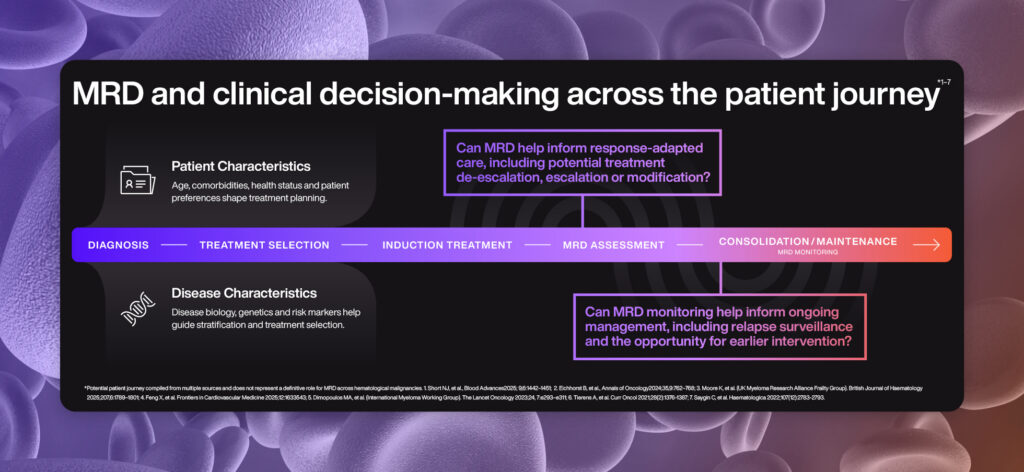
Care has to fit the whole patient, not just the disease. In this context MRD does not replace clinical judgement, but provides an additional parameter that must be interpreted alongside disease biology, treatment context and the patient preferences.7–9
Treatment strategies will consider patient age, comorbidities, lifestyle and treatment preferences, and establishing the genetic characteristics of disease informs risk stratification that guides treatment selection from the outset, based on established clinical data.7–12
However, taking advantage of MRD monitoring clinicians are increasingly able to move from one-size-fits all treatment, to adaptive care where treatment intensity, modality and duration can be personalized to fit disease behavior, this extends to monitoring for signs of relapse.4
What are the current limitations for MRD in hematology?
The role of MRD is continually being defined and it’s important to understand that MRD isn’t equally validated across the hematology landscape. The prognostic impact of MRD is established in acute lymphoblastic leukemia, where it is already incorporated in treatment protocols and can drive treatment decisions,7 in chronic lymphocytic leukemia, MRD is being investigated in the context of fixed-duration therapy.13
However, across the field, challenges remain in standardization of assays, thresholds used for confirming MRD and interpretation of the evidence.4 Disease heterogeneity remains core to interpretation and application of MRD. Negativity does not mean cure. Patients may be at risk of relapse and in some cases where patients have a low risk of progression, and it is important to consider MRD in context of disease control vs. the risk of over-treatment.4
What does the future hold?
There is much to look out for in the coming years as the landscape continues to evolve. Regulators are engaging with MRD as a surrogate trial endpoint. For example, in 2024 a US FDA advisory committee voted that MRD can support accelerated drug approval in multiple myeloma.14The acceptance of MRD-negative complete response as an earlier, surrogate endpoint may help streamline and reduce the required duration of clinical trials by half in some cases, presenting the opportunity to bring effective therapies to patients sooner.14
As the field continues to evolve, EHA provides an opportunity to take stock of where MRD is heading. We will be following emerging data from MRD-guided trials and progress in standardization efforts alongside the evolution of technologies. There is also growing interest in how AI and multi-omic approaches may complement MRD to create a richer picture of disease biology and treatment response.
Underpinning many of these discussions is a broader question: how can increasingly sensitive measures of disease be translated to clinical decision making for the benefit of patients?
Interested in how advances like MRD are changing the hematology landscape?
Get in touch with the Real Chemistry Medical Communications team to explore how scientific communications can help turn emerging evidence into clinical understanding, confidence and action.
References
- Khoury R, et al. Biomedicines, 2025:13,7;1654.
- European Hematology Association, 2026. 11–14 June 2026, Stockholm, Sweden https://ehaweb.org/connect-network/eha2026-congress
- Yoroidaka A, et al. Haematologica, 2025:110,9.
- Chandhok NS, Sekeres MA. eClinicalMedicine, 2025:86;103348.
- Forghani F, et al. npj Precision Oncology, 2025:9;385.
- Landgren O, et al. Blood, 2024:144,4;359–367.
- Short NJ, et al. Blood Advances, 2025:9,6;1442–1451.
- Eichhorst B, et al. Annals of Oncology, 2024:35,9;762–768.
- Moore K, et al. British Journal of Haematology, 2025:207,6;1789–1801.
- Feng X, et al. Frontiers in Cardiovascular Medicine, 2025:12;1633543.
- Dimopoulos MA, et al. The Lancet Oncology, 2023:24,7;e293–e311.
- Tierens A, et al. Curr Oncol, 2021:28(2);1376–1387.
- Brown RJ, et al. N Engl J Med 2025;392(8):748-762.
- Landgren O, Devlin S. Blood Cancer Discov., 2024:6(1);13–22.


